How Dry Needling Can Help with Frozen Shoulder (Adhesive Capsulitis): A Science-Backed Approach to Pain…
Tennis Elbow: How Sports Acupuncture Can Help!
Tennis elbow got its name because the condition was first commonly observed in tennis players, especially those who played with poor technique or used a heavy or tightly strung racket. It became popular in the early 20th century when doctors noticed a surge in cases among tennis players. The condition, “lawn tennis elbow”, was first described in medical literature in 1873 by British surgeon Henry Morris (Labelle, 1992).
Tennis elbow, medically known as lateral epicondylitis, is a condition that causes pain and inflammation around the outside of the elbow from tiny microtears and degeneration (tendinosis) in the tendon of the forearm muscle attached to the bony bump (lateral epicondyle). The extensor carpi radialis brevis (ECRB) is the muscle most involved in tennis elbow. It helps stabilize the wrist during gripping and extension motions. It most often affects the dominant arm and is particularly common in people between the ages of 30-50 years (Shiri, 2006).
What Causes Tennis Elbow?
Despite the name, you don’t have to play tennis to get tennis elbow. Today, of those who suffer from tennis elbow only 5% of cases are from playing tennis (Coombes, 2015). Of that 5% of tennis players, left-handed players tend to have a lower incidence of tennis elbow, possibly because they face fewer right-handed spin-heavy shots that stress the elbow.
Tennis elbow is now more often seen in people who do repetitive arm and wrist motions like carpenters, painters, plumbers, butchers, musicians, or office workers using a mouse and keyboard. Even common tasks such as gardening and knitting can cause tennis elbow. It’s the repetitive stress or overuse of gripping and twisting. As an interesting sidenote: in Japan, it’s often called “washerwoman’s elbow” due to its prevalence in people doing repetitive handwashing.
Athletes Who Experienced Tennis Elbow
Not all athletes who experience tennis elbow are tennis players. Alex Honnold, an elite rock climber dealt with elbow and forearm tendon stress, especially from gripping and pulling. Kobe Bryant experienced chronic elbow pain from overuse, especially due to repetitive shooting motions and weight training. Mark Messier, a hockey player, battled with elbow tendon issues related to repetitive stick handling and shooting. John Smoltz, the baseball pitcher had elbow tendonitis affecting his pitching arm. Phil Mickelson, the famed golfer, experienced symptoms consistent with golfer’s elbow, a close cousin to tennis elbow, caused by repetitive golf swings. Tiger Woods revealed he was suffering from tennis elbow, which caused him pain during the U.S. Open and forced him to skip the AT&T National tournament. *
Tennis elbow has affected these great tennis players: Pete Sampras, reportedly struggled with elbow pain during his career. Novak Djokovic, sidelined by persistent elbow injury that eventually required surgery in 2018. And, no tennis list would be complete without mentioning Serena Williams, who experienced elbow inflammation and pain during her career, noted during the 2015 French Open, which she attributed partly to a change in her racket.*
*Tennis Elbow vs. Golfer’s Elbow
| Condition | Location of Pain | Affected Tendons |
| Tennis Elbow | Outer elbow (lateral) | Wrist extensor tendons |
| Golfer’s Elbow | Inner elbow (medial) | Wrist flexor tendons |
Treatment Options
Conservative – First Line
Allow the condition to resolve without active medical intervention, relying on the body’s natural healing processes, especially in the early states or when symptoms are mild. Up to 80-90% of cases improve within 6-24 months, naturally (Coombes, 2009). This involves avoiding aggravating activities (like gripping, heavy lifting, racquet sports), applying ice for pain relief as needed, gentle stretching if tolerated, the use of NSAIDs – medications that relieve pain, inflammation, and fever, physical therapy, and bracing or elbow straps.
Alternative Therapies
- Traditional Acupuncture – May help reduce pain and improve function (especially helpful in chronic cases).
- Corticosteroid Injections Corticosteroids – Short-term relief, but high recurrence risk and potential tendon weakening.
- Shockwave therapy (ESWT) – Uses sound waves to stimulate healing, shows some benefit in chronic cases by stimulating healing and desensitizing pain receptors.
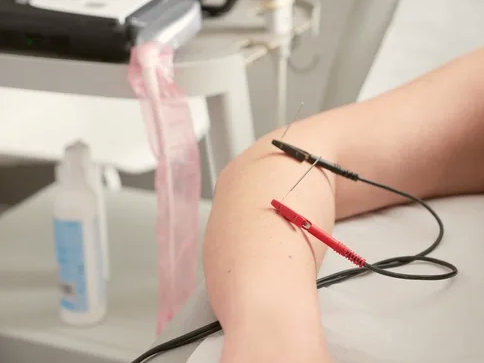
- Dry Needling/Sports Acupuncture – Stimulates blood flow and promotes tissue repair; increasingly used with positive outcomes.
- Massage therapy – Especially deep tissue massage to release tight muscles and tendons.
- Surgical Treatment – Considered only after 6–12 months of failed conservative management.
Preventive Measures
Preventive measures include using ergonomic tools or equipment, improving technique if playing sports or using tools repetitively, strengthening forearm, should, and wrist muscles to prevent recurrence.
Strengthening exercises to try at home: wrist extension with light weights, wrist supination/pronation, and a towel twist.
Conclusion
Tennis elbow is a common, self-limiting tendon condition that affects the outer part of the elbow due to repetitive strain, especially involving the wrist extensor muscles. In most cases, the condition resolves naturally over time—with research showing that 80–90% of individuals recover within 6 months to 2 years, even without formal treatment.
While “letting nature take its course” is often sufficient in mild cases, evidence suggests that active rehabilitation—particularly eccentric exercise and manual therapy—leads to faster, more complete recovery and reduces the risk of recurrence. Injections and surgery are generally reserved for chronic or resistant cases.
Ultimately, the best approach is an individualized plan based on symptom severity, functional limitations, and personal goals. Early care and activity modification support healing, while persistent or disabling symptoms benefit most from structured intervention.
References
Coombes, B. K., Bisset, L., & Vicenzino, B. (2009). Management of lateral elbow tendinopathy: One size does not fit all. Journal of Orthopaedic & Sports Physical Therapy, 39(3), 200–209. https://doi.org/10.2519/jospt.2009.2835
Shiri, R., Viikari-Juntura, E., Varonen, H., & Heliövaara, M. (2006). Prevalence and determinants of lateral and medial epicondylitis: A population study. American Journal of Epidemiology, 164(11), 1065–1074. https://doi.org/10.1093/aje/kwj325
Bisset, L., Beller, E., Jull, G., Brooks, P., Darnell, R., & Vicenzino, B. (2006). Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: Randomised trial. BMJ, 333(7575), 939. https://doi.org/10.1136/bmj.38961.584653.AE
Labelle, H., Guibert, R., Joncas, J., Newman, N., Fallaha, M., & Rivard, C. H. (1992). Lack of scientific evidence for the treatment of lateral epicondylitis of the elbow: An attempted meta-analysis. Journal of Bone and Joint Surgery – British Volume, 74(5), 646–651. https://doi.org/10.1302/0301-620X.74B5.1388172
Curated, compiled and written by Dr. Nathan J. Heide, DAOM, MBA, LAc and Rebecca Carsten to offer an insightful overview of sports acupuncture, dry needling, and medical topics in Eugene, Oregon
Related Posts


